Immuno-oncology (IO) therapy is a new (and old) way to treat cancer by activating your immune system in the hope that it will attack your tumour.
One of the earliest treatments for cancer was a kind of immune therapy. Over a century ago, the American physician William Coley concocted a soup of bacterial toxins that was injected directly into tumours. The so-called “Coley’s Toxins” caused a great deal of inflammation and unfortunately sickness but did cure of a small number of people, and were used as treatment until well into the 1960s. Since then, a number of other immune therapies have been developed and trialled over the last century, but until recently side effects, cost and variable benefits have limited their usefulness.
Powered by our expanding knowledge of the cellular mechanisms of the immune system, newer types of immune therapies (also called immuno-oncology or IO therapies) have been proving successful in some types of cancer, including kidney cancer. Other types of immune therapies including vaccines are currently in trials for kidney cancer.
In this section, you will learn about which IO therapies effective for kidney cancer, how they work and what their side effects might be. To understand the new IO therapies it is important to know how our immune system works. If you want to learn more about our immune system, please read here first: How does the immune system work
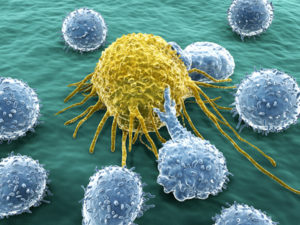
Lymphocytes attacking cancer cell
Our immune system is able to recognise cancer cells as abnormal, and is sometimes able to mount an effective response against the cancer. In very rare cases of melanoma and kidney cancer, this can lead to a spontaneous remission, a miracle cure of the cancer. However, cancers are able to grow in the first place by making themselves invisible to the immune system, blocking anti-cancer signals that would otherwise cause the immune system to attack. The goal of immunotherapy is to activate, strengthen and support the body’s immune system against cancer.
There are several kinds of immune therapies available (and being tested) for many types of cancer:
1. Vaccines directed at cancer
Vaccines have been tested in many types of cancer, but older vaccines have mostly been ineffective in treating cancer to date. Trials are ongoing with new types of cancer vaccines. The most vigorous area of investigation are personalised therapies that use tissue from a patient’s tumour to create a customised vaccine for directing the immune system on targets expressed by their own cancer cells.
Note: Other hugely important immune-therapy vaccines are those that can prevent the viruses that cause specific cancers (such as hepatitis B and HPV – the human papilloma virus). These vaccines prevent hundreds of thousands of cancers around the world every year.
2. Cytokines (immune hormones)
The immune system communicates by hormones (e.g. interleukin and interferon). Large doses of these given as injections have been used to treat some kinds of cancer including kidney cancer.
3. Immune cells harvested and expanded out of the body
A person’s own immune cells (their lymphocytes) can be harvested from their body, and expanded outside the body and reintroduced. These include tumour infiltrating lymphocytes (TILs) and with further modification chimeric antigen receptor (CAR) T-cell therapy.
4. Checkpoint antibodies
So called monoclonal antibodies have been developed to disrupt the handshake between immune cells and their targets. This is a rapidly developing field for immune therapy of cancer.
Clinical trials are exploring how to personalise treatment based on the exact characteristics of your tumour. Some clinical trials request a biopsy or specimen of your tumour. Researchers are hoping to determine which types of cancers might be most receptive to IO therapies.
At the moment there are four types of IO therapy being used and tested for kidney cancer:
1. Cancer vaccines (e.g., dendritic cell vaccines, others)
 Vaccines have been tried in kidney cancer. One vaccine seemed to be successful in preventing the cancer recurring in patients who had a large cancer removed from their kidney. This was a complex process however and this vaccine has not become a standard treatment.
Vaccines have been tried in kidney cancer. One vaccine seemed to be successful in preventing the cancer recurring in patients who had a large cancer removed from their kidney. This was a complex process however and this vaccine has not become a standard treatment.
Vaccines being tested in kidney cancer trials include:
- AGS-003: samples of your immune cells are collected and then genetically modified so that they recognise your tumour cells. Your modified immune cells are injected back into you. This is similar to CAR therapy, except that in this case the injected cells do not fight the tumour, but instead teach your adaptive immune system to fight it. This study did not show an improvement in outcome and is unlikely to become a standard treatment for kidney cancer.
- IMA901: this vaccine contains 10 common kidney cancer proteins. It works in a similar way to a normal vaccine, so it will not make you ill, but it is designed to teach your immune system how to recognise your tumour cells. IMA901 did not show a survival advantage to standard sunitinib treatment and will not be a standard treatment for kidney cancer.
- MGN1601: this vaccine contains someone else’s kidney cancer cells. When you are injected with the vaccine, your immune system will destroy these cells because they do not belong to you and will be recognised as a threat. While your immune system is fighting these foreign kidney cancer cells, it will also learn what a kidney cancer cell looks like and will therefore be able to destroy your tumour. This agent is still undergoing study.
2. Cytokine therapy (immune hormones for unspecified immune stimulation, e.g., IL2, IFN)
Before targeted therapies became available to patients with kidney cancer in 2006, some people were treated with immune hormones such as interleukin-2 (IL-2) and interferon-alpha (IFN). Some people who were given this older type of immuno-therapy responded very well to this treatment. Some people even had a durable complete response, meaning that the cancer went away completely and they have had a very long-term benefit from the treatment.
It is hard for doctors to use the word “cured” in this situation, but some people have lived a very long time after treatment. On the other side of the coin these immune hormones are extremely toxic; only young, physically fit people can take them, and even then people are so sick they are usually treated in intensive care units.
3. Immune cell therapy (e.g., T-cell infusion therapy or TILS)
These types of therapies are currently in clinical trials for some types of cancer, but are only available in a few major research institutions worldwide.
4. Checkpoint antibodies (e.g., CTLA-4, PD-1, PD-L1)
Checkpoint immune therapy is the most recent development in the immune therapy of kidney cancer. Many clinical trials are underway around the world that are either specifically for kidney cancer, or that include kidney cancer in the selection criteria, and several agents are now approved.
Immune cells are controlled by a committee of checkpoints which very finely balance the immune system. Too little regulation and the immune system goes overactive and attacks the body; too much and immune functions are impaired and infections and cancers can establish themselves.
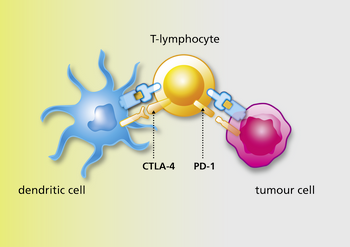 Sometimes cancer cells co-opt this system and use checkpoints inappropriately to stop your immune system recognising cancer cells. Checkpoint inhibitors are drugs (in this case antibodies) that in turn block these checkpoints so that the immune system is freed up to fight cancer cells.
Sometimes cancer cells co-opt this system and use checkpoints inappropriately to stop your immune system recognising cancer cells. Checkpoint inhibitors are drugs (in this case antibodies) that in turn block these checkpoints so that the immune system is freed up to fight cancer cells.
Understanding how these checkpoint antibodies work explains a lot about how they do (and don’t) work in cancer patients. For example, checkpoint immune therapy does not seem to help unless the immune system is already targeted, alerted, activated and attempting to infiltrate that cancer.
Researchers are still learning who will be and who won’t be helped, but it does seem that if there are no immune cells inside the tumour, then the checkpoint antibodies may not work. Understanding that checkpoint antibodies only lift the last line of the cancer’s defence against the immune system also explains the strategy that doctors and scientists are taking forward in clinical trials.
This work resulted in the US Food and Drug Administration (FDA) approval of nivolumab, a PD-1 blocking antibody, in 2015 for metastatic kidney cancer in the second-line setting, with subsequent approval in Europe and other parts of the world. Additionally the combination of nivolumab and ipilimumab, an antibody against CTLA-4 was US FDA approved in April 2018.
The development and availability of checkpoint antibodies for different cancers has been one of the most rapid stories in medical history. It has been a whirlwind of activity and new findings are published every month.
 First and foremost, patients should seek advice from an expert in kidney cancer to determine whether immuno-oncology treatment is appropriate for them.
First and foremost, patients should seek advice from an expert in kidney cancer to determine whether immuno-oncology treatment is appropriate for them.
Kidney cancer experts can best advise you on various ways to access immuno-oncology therapies for kidney cancer. Depending upon your country, these methods may include:
Obtain IO agents through your health care system
Nivolumab and the combination of nivolumab and ipilimumab may be available through your health care system in your country. Check with your physician team to determine what is available to you at this point in time.
Join a clinical trial
Different types of IO therapy for kidney cancer are being actively researched in clinical trials. This website maintains a list of current IO clinical trials for people with kidney cancer. Trials included are those operating in more than one hospital or recruiting a significant number of patients. Smaller trials might also be available at your hospital. Some are in the final phases (Phase 3). If these trials are successful, the first medications may be approved for use.
However, depending upon your country, the clinical trial and approval processes can take some time so it may be several years before any type of IO therapy becomes widely available. In the meantime, new trials are expected to answer important questions specific to kidney cancer.
Seek Compassionate Access Programs
Some checkpoint antibodies may be available on compassionate grounds. Some companies have established compassionate access programs, or expanded access programs where doctors can apply for early access to drugs. This is complex, varies by country, is subject to change at short notice and requires a lot of paperwork. The patient organisation in your country may know which compassionate access programs are available. For information on patient organisations near you, please check “our global network“.
Obtain through Private Insurance or Personal Funds
The cost of these new drugs is very high. Estimated costs could be as much as $150,000 U.S. for one year. Insurance companies might or might not cover the cost of these medications. Depending upon your country’s regulations, you might or might not be able to pay for the drug personally and have it infused. Be sure to speak to your physician before paying out of pocket for the medication to ensure that there are no clinical trials or compassionate access programs that you could benefit from.